Healthcare UX
Service Design
Al Prototyping

About the project
To say that Canada has a healthcare crisis is an understatement.
28,000 people died waiting for a medical procedure or diagnostic.
6.5 million Canadians don’t have a family doctor.
16.1 million unscheduled Emergency Department visits in 2024 - 2025, an increase from 15.5 million the year before.
In this environment, small bottlenecks create outsized impact, especially at the ER.
The Problem: A System Near Breaking Point
Emergency departments nationwide are overwhelmed.
Patients wait an average of 4 hours from arrival to discharge, and 1.2 million leave without receiving treatment at all.
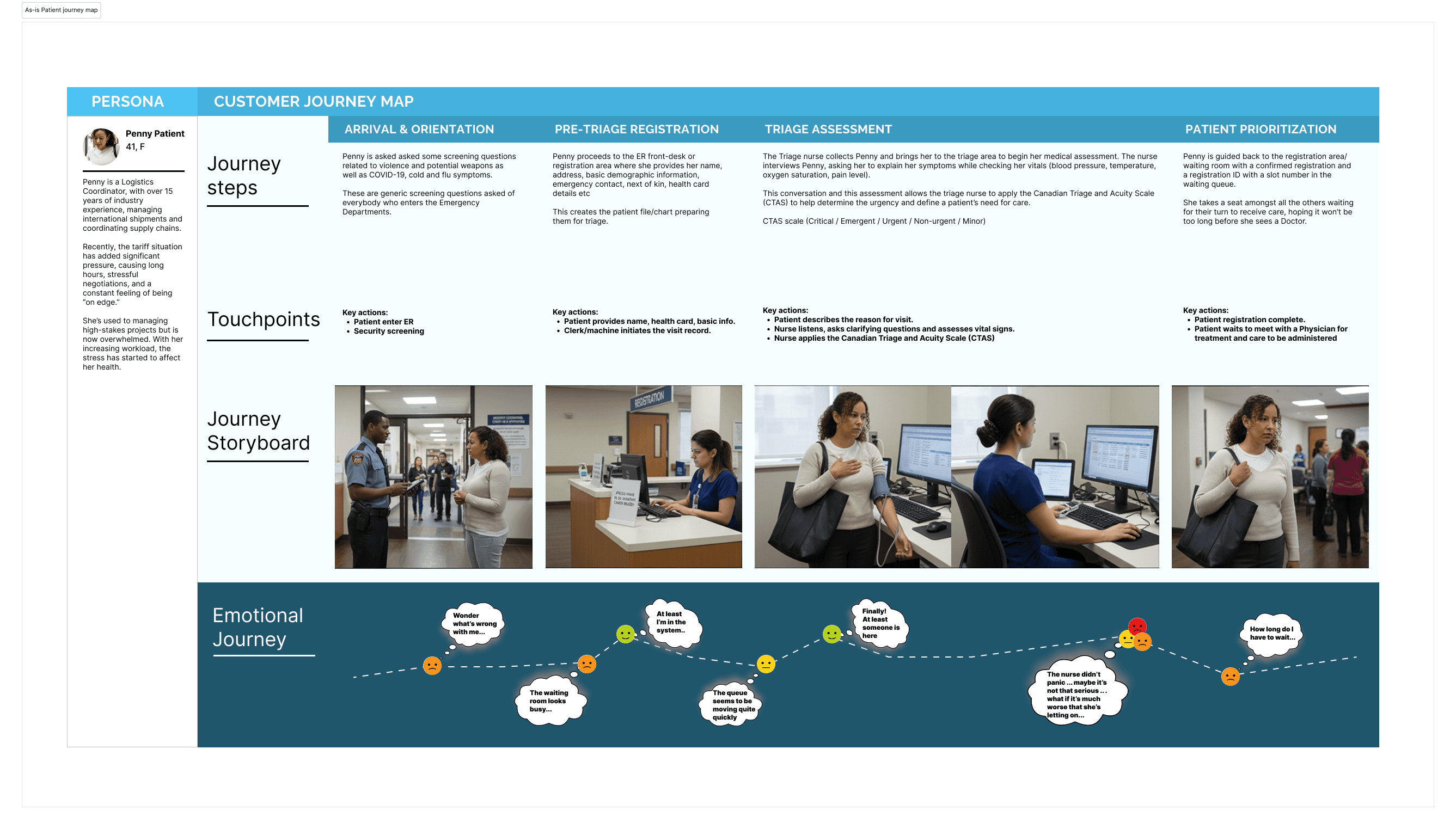
The first interaction (registration and triage) sets the tone for the entire patient journey. Today, that process is:
entirely manual
error-prone
slow & inefficient
inconsistent across staff and sites
The result:
Patients feel anxious and uninformed. Nurses are overburdened with clerical work, pulled away from clinical care. Data inaccuracies cascade through the care episode.
The Challenge: A system stalled from all sides
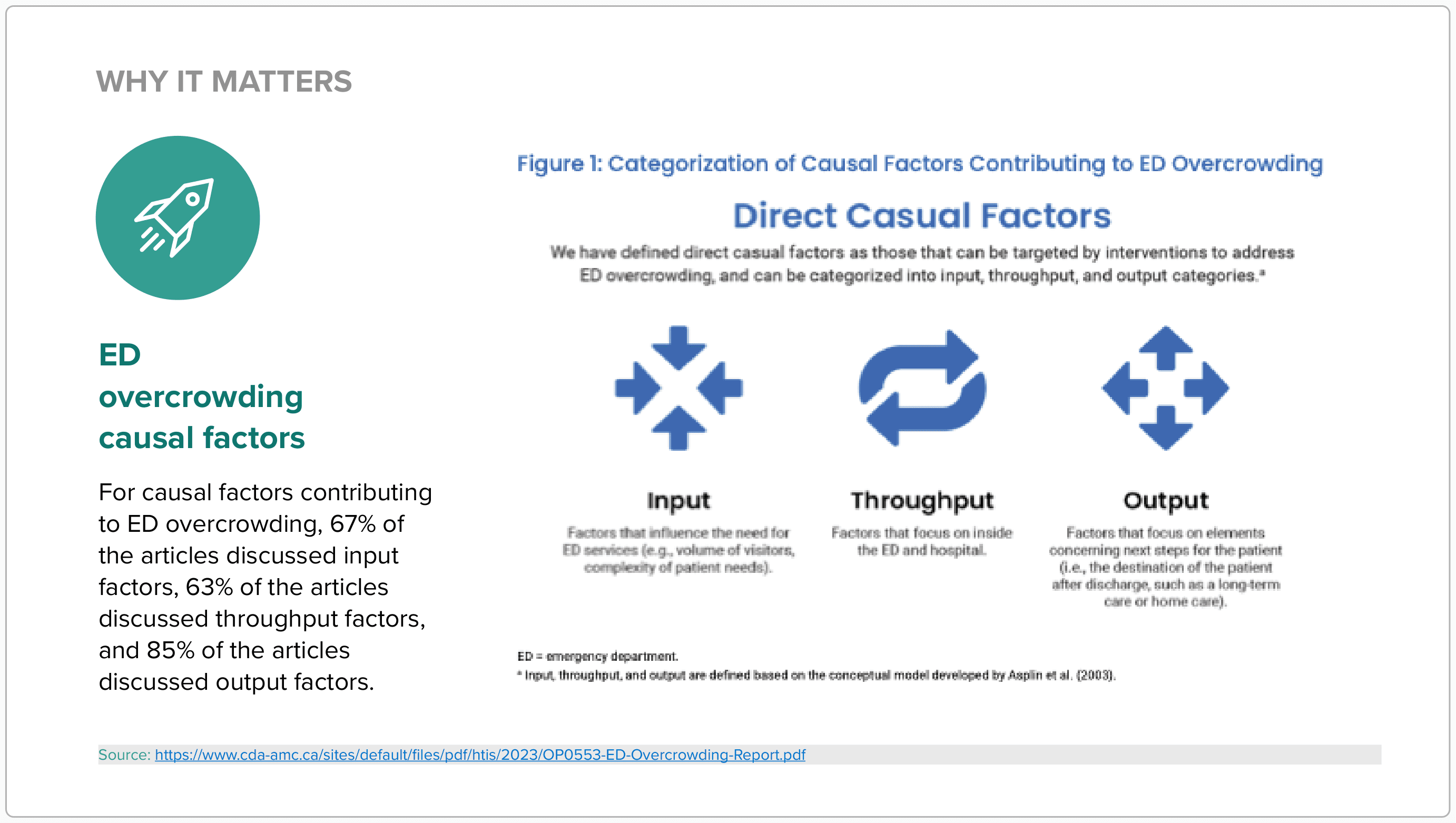
ER overcrowding isn’t caused by a single failure point; it’s driven by pressures that can be broken down across input, throughput, and output. A 2023 assessment shows:
67% of studies cite input pressures (more patients, more complex needs)
63% cite throughput pressures (in-hospital workflow delays)
85% cite output pressures (no beds, no discharge destinations)
Multiple interconnected factors at the interface of the ED; today’s front door registration and triage, sits exactly where these forces collide. Through primary and secondary research, we were able to recognize and validate:
The growth of input pressures
ER patients are arriving sicker, older, and with more complex needs.
CTAS Levels 2 & 3 (urgent / emergent care) have been steadily increasing for more than a decade.
More patients require rapid intervention.
Older adults (65+) now represent a growing portion of total ER visits.
Median wait time to physician initial assessment continues to rise.
Unresolved complexity at the intake stage means manual workflows break faster, data errors carry more risk, and triage inconsistency becomes more dangerous.
The slowdown of throughput
Once inside the ER, everything moves slower:
Median length of stay continues to increase.
Documentation demands and repeated information gathering slow down clinical teams.
Without efficient digital intake, clinicians are forced to compensate manually, multiplying delays throughout the entire system.
The resultant bottleneck of output
Fewer patients are being discharged directly from the ER.
The proportion of patients leaving without being seen continues to climb.
This cascading output blockage pushes the entire queue backward, right to the front door, where registration and triage get overwhelmed. Thus the first step is the biggest brake, the biggest opportunity, with the most critical pain points:
Queue congestion forms even before clinical care begins
Nurses spend up to 60% of triage time on repetitive clerical tasks
CTAS prioritization varies, creating risk of over- or under-triage
Lack of transparency leaves patients confused and unsettled
Over 50% of level 3 patients revisit the ER within 7 days of their first visit.
The Opportunity: A High-ROI Fix With System-Wide Impact
Digitizing intake and triage can:
Cut wait times by up to 60%
Improve CTAS accuracy with AI-assisted decision support
Reduce clerical burden and nurse burnout
Give patients live updates on their position in queue
Improve data quality and downstream workflows
Strengthen trust and transparency from the moment a patient arrives
This isn’t just about upgrading the user experience or a shiny new user interface; it’s a systems intervention with the potential for measurable improvements across the board.
How might we design a digital intake and triage experience that reduces nurse workload, improves triage accuracy, and creates transparency for patients; without disrupting clinical workflows?
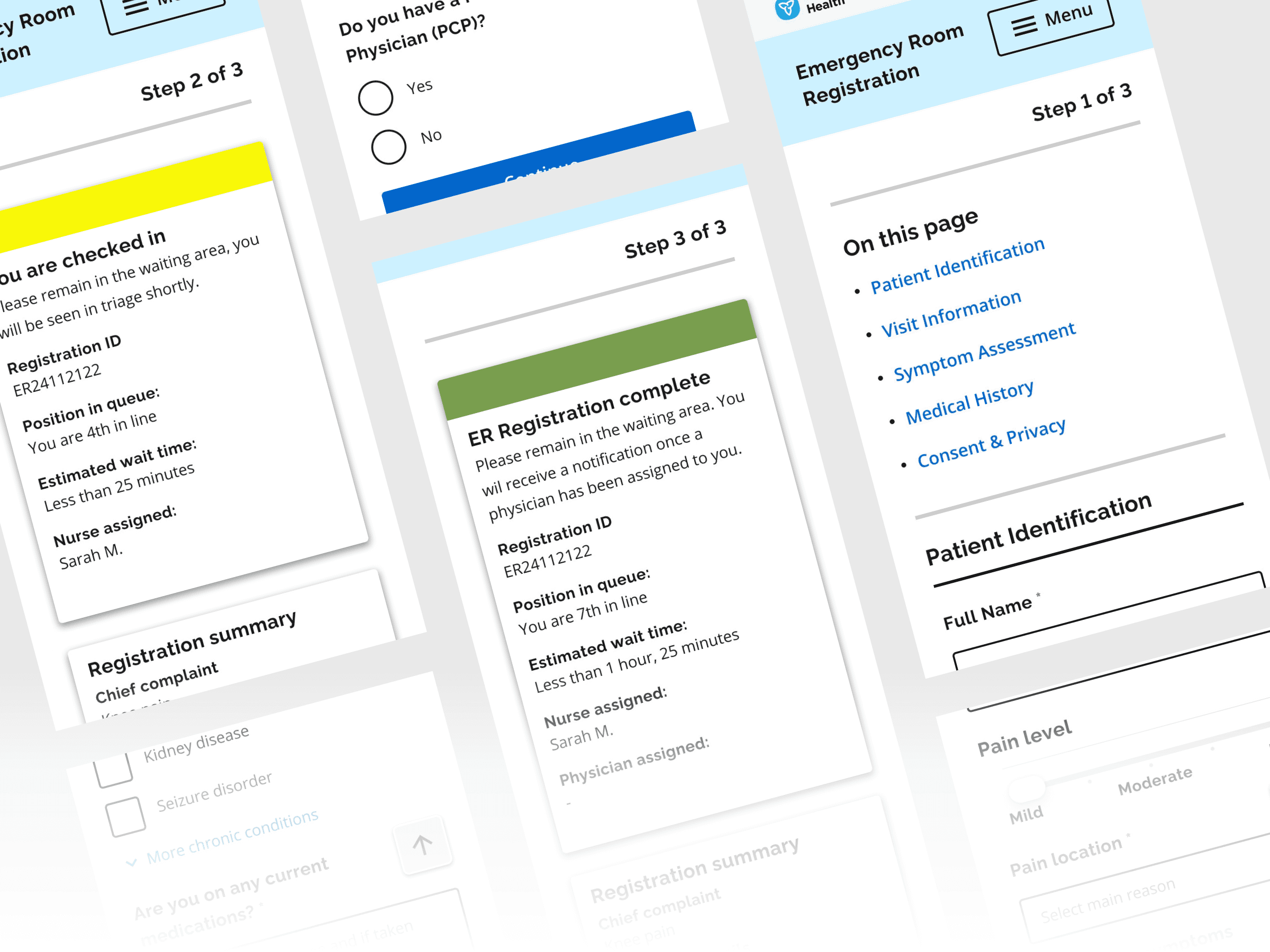
The Solution: A Digital Intake & AI-Enabled Triage Platform
Digital Registration
Mobile-first, responsive form accessible via QR, kiosk, or portal
Captures demographics, insurance, medical history, and symptom details
Patients confirm their own data → fewer errors
Electronic Triage Assessment
Structured questionnaire aligned with CTAS
Guided capture of vitals, pain level, red flags
Automated documentation reduces cognitive burden
AI-Suggested CTAS Level
Model trained on Ontario’s 6M+ ER visit dataset
Recommends acuity level; nurses retain full override authority
Audit trail ensures accountability
Real-Time Journey Updates
Dynamic wait-time estimates
Staff notifications triggered by acuity thresholds
Full visibility from registration → triage → treatment → discharge
Enterprise-Ready Architecture
WCAG 2.1 AA accessibility
HIPAA & PIPEDA compliant
Real-time EMR integration (no duplicate entry)
Analytics dashboard to identify bottlenecks & demand trends
Client
Ontario Health
Stack
Figma Lovable Supabase
Role
Lead Product Designer
Year
2025



Visuals



